Across the country, just 10% of community-based palliative care programs are spearheaded by home health care providers. The coronavirus may change that moving forward.
As of Monday, there have been more 1.9 million confirmed COVID-19 cases in the United States, with many individuals in recovery. But while some see a return to full health, doctors are also starting to notice a growing list of lasting health impacts, including heart, kidney and brain problems.
If secondary and tertiary complications prove common and long-lasting, that may lead to higher demand for advanced illness care, particularly for the senior population. It’s a trend that Capital Caring is already seeing, Dr. Matthew Kestenbaum, the organization’s chief medical officer, told Home Health Care News.
“Right now, we are seeing from our hospital partners and our community colleagues the importance of palliative care, including advanced care as well as appropriate pain and symptom management,” Kestenbaum said. “The number of palliative care consults we’re being asked to perform in the hospitals and in the community has actually increased. The importance of palliative care is absolutely being shown during this pandemic.”
Falls Church, Virginia-based Capital Caring is one of the largest nonprofit providers of advanced illness, hospice and at-home care for seniors in the Mid-Atlantic region. As one of the country’s original hospice demonstration sites, the company cut its teeth in end-of-life care but has since expanded into various services aimed at aging in place.
Overall, Capital Caring helps treat more than 2,000 people on a daily business across its services lines.
“We have really expanded our services after originally starting out as a hospice program,” Capital Caring President and CEO Tom Koutsoumpas told HHCN. “Our goal is to continue providing care across the continuum in order to help people stay at home. Whether that’s providing advanced illness care [or] home-based primary care — we’re doing whatever we can do to help individuals age in place.”
In addition to his CEO role at Capital Caring, Koutsoumpas is also the co-founder of both the Coalition to Transform Advanced Care (C-TAC) and the National Partnership for Hospice Innovation (NPHI).
Palliative and advanced illness care have arguably never been more in the spotlight than during the current public health emergency.
In fact, one recent op-ed in the Journal of Cardiopulmonary and Acute Care argues that palliative care principles should guide the care that all COVID-19 patients receive.
Broadly, the core aspects of palliative care can provide a foundation for responding to COVID-patient needs, including symptoms alleviation, multidisciplinary teams, patient-centered care and family support.
Capital Caring has been working to strengthen those core principles across its markets.
“We … have been very willing to work with our community partners, in terms of helping to guide symptom management, grief and loss counseling — not only for families of patients who have died from COVID, but for staff who’ve been taking care of them who are just not used to this degree of acuity or loss,” Kestenbaum said.
On its end, Capital Caring started closely following the coronavirus situation in February, then took action in the beginning of March. Its early response strategy included the formation of a dedicated leadership team focused on developing best practices and protocols.
The company also acted quickly to secure as much personal protective equipment (PPE) as possible while simultaneously shifting operations to virtual platforms.
“We’re using Zoom [for virtual meetings],” Kestenbaum said. “We considered a couple options, but … we were able to get that in place in a matter of two or three days. By the third week in March, all hospice team meetings were virtual. Only necessary home visits were being made — and we still did those very quickly.”
Nationally, 33% of palliative care programs are operated by hospice providers, 32% by hospitals, 14% by office practices or clinics, 11% by long-term care facilities and 10% by home health agencies, according to a 2019 report from the Center to Advance Palliative Care (CAPC).
If home health providers don’t have experience in advanced illness or palliative care, they should turn to organizations like Capital Caring for support, Koutsoumpas said.
“Partnering with hospice and palliative care providers in the community is important,” he said. “Encouraging these kinds of relationships can really expand the ability to care for people in the community.”
A handful of home-based care providers have already signaled plans to expand into palliative care.
CareCentrix — a care management company that focuses on home-based care — announced in May it had acquired palliative care company Turn-Key Health for an undisclosed sum.
Paul Kusserow, president and CEO of Amedisys Inc. (Nasdaq: AMED), also recently hinted that palliative care may be in his company’s future.
“We’re primarily in home health and hospice now, but we’re moving forward into personal care and expanding into palliative care, which we believe is becoming increasingly important,” Kusserow previously told HHCN.
For seniors recovering from the coronavirus, home health care aides have provided another way to care for at risk adults that might otherwise need to be in a nursing home or adult care facility.
Both Gov. Andrew Cuomo and Mayor Bill De Blasio have called for an increase in home care to help keep seniors out of the hospital and even help slow the spread of the virus in nursing homes.
What You Need To Know
o Home health aides need more support.
o Older New Yorkers are especially vulnerable to COVID.
o Home health aides themselves have also died.
o Home health aides’s work can help free up needed hospital space.
“If I were advising a friend, I would say: You have a vulnerable person. Best to keep them at home and not put them in a congregate facility,” Cuomo said during an interview on MSNBC. “Keep them in a situation where you have the most control and that is the blunt truth.”
But home health care aides have not been left untouched by the virus.
A survey of six home care agencies showed that 780 home health care aides caught COVID-19 and 33 home aides have died.
However, these six agencies were also able to take care of 20,000 at risk adults during the past few months, keeping them home and out of the hospital system.
“By discharging them from the hospital, back home and skipping the step of the nursing home or rehab has really saved, I think, countless lives,” siad Michael Arnella, RN, the director of Clinical Services at Accent Care.
Arnella continued, “And then with the hospitals around 80% COVID at one point, having these other patients go in with DHS, DOPD, diabetes, would overwhelm the system. Home care plays a vital role in any type of emergency situation.”
By Morgan McKayNew York State PUBLISHED 5:27 AM ET Jun. 02, 2020 Source: Spectrum News
Family health care decision-makers have followed the devastating effects that the COVID-19 virus has had on the long-term care facilities. That experience is now pushing them toward home-based care, new data suggests.
Over 50% of family members are now more likely to choose in-home care for their loved ones than they were prior to the coronavirus, according to a recent survey from health care research and consulting firm Transcend Strategy Group.
As part of its survey, Transcend reviewed feedback from about 1,000 respondents, all of whom were family health care decision-makers. Broadly, those decision-makers were more likely to be women between the ages of 40 and 45 years old.
“One of the biggest takeaways … was that 65% of respondents agreed that COVID-19 had completely changed their perception about the best way to care for aging seniors,” Stan Massey, a partner at Transcend Strategy, said Wednesday during a National Association for Home Care & Hospice (NAHC) webinar. “I’ll give you a little spoiler alert: That mind-shift has landed squarely in the favor of home-based care providers.”
Nearly half of survey participants said they had previously considered placing a loved one in a long-term care facility in the future, but have now taken that option off the table.
Additionally, despite the home-based care arena’s own struggles with procuring personal protective equipment (PPE), survey respondents were still overwhelmingly confident that in-home caregivers were following necessary protocols during COVID-19.
In all likelihood, the shift in thinking is not temporary. Within the survey, respondents suggested that their perception of the long-term care options had been changed for good.
“COVID-19 has changed opinions from this point forward,” Massey said. “It had such an impact on families that we feel this ripple effect of really wanting to take every precaution, even if a vaccine for COVID-19 does emerge.”
The concerns are driven, in large part, due to the staggering death toll in facilities across the U.S. Newly released federal statistics show nearly 26,000 people have died from COVID-19 in nursing homes through May.
Family decision-makers’ newfound appreciation of home-based care will likely offer future opportunities for providers looking to grow their businesses.
LHC Group Inc. (LHCG) Chief Strategy and Innovation Officer Bruce Greenstein echoed a similar sentiment Tuesday during a presentation at the Jefferies Virtual Healthcare Conference.
“[The coronavirus is going to change] the psyche of the way people are going to view … long-term care facilities for the rest of our generation,” Greenstein said.
Harnessing momentum
In tandem with family members’ bullishness on home-based care is their increased interest in the value of telehealth.
Over 60% of individuals who participated in the Transcend survey said they’re likely to explore telehealth options in the future.
Telehealth claim lines in the U.S. increased 4,347% between March 2019 and March 2020, according to FAIR Health’s Monthly Telehealth Regional Tracker. A claim line is an individual service listed on an insurance claim.
Though the Centers for Medicare & Medicaid Services (CMS) has not yet authorized the ability for home-based care agencies to be reimbursed for telehealth as they would be for in-person visits, restrictions on remote patient monitoring have been eased. The agency has loosened some of the red tape surrounding virtual care and has encouraged its use during the COVID-19 outbreak.
“When the restrictions started being [removed] off of telehealth, we really thought that it was like letting the genie out of the bottle. And it’s only going to improve from here,” Massey said.
Even if a provider is unable to bill for telehealth services, having good telehealth practices in place could increase the likelihood of a client initiating care plans with them.
“Even if you’re not able to be reimbursed for the delivery of care through telehealth, be thinking holistically about how you deliver adjacent values,” Transcend CEO Stephanie Johnston said on the webinar. “There’s a lot more openness and flexibility within the regulatory framework now for home health providers to get really creative and innovative.”
For the first time in our modern history, staying at home has become a “new” normal. And with more than 1.5 million Americans now infected with COVID-19, never before in our lifetime has accessing care in a person’s home been so important.
Smartly, our federal and state policymakers quickly expanded reimbursement for telehealth and removed barriers that have now allowed more providers to care for patients virtually via video and phone, eliminating the risk of COVID-19 exposure during provider visits. But not all care can be provided through telehealth – and we would be shortsighted to not also address the growing need for home-based care.
Long before the COVID-19 emergency, health care policy experts have increasingly recognized the value of home-based health care. A recent AARP survey found that three in four adults 50 years and older would prefer to age in their homes and communities. And a growing body of evidence suggests it is less expensive to deliver care in the home. Indeed, for years we’ve seen hospitalized patients more quickly returning to their homes and communities to heal and recover safely, reducing costs for themselves and the health care system.
Home-based care addresses some of the negative health effects of social isolation and loneliness, which drive poorer health outcomes that annually cost billions of excess health care dollars. According to one study, those experiencing loneliness and social isolation had a more than 60 percent higher risk of developing dementia and a fourfold increase in hospital readmission rates within a year of discharge.
Despite its demonstrated value, our country has yet to fully integrate the support needed for home-based care. Instead, we have a collage of different reimbursement frameworks across state, federal, and private payers.
Traditionally, Medicare has paid only for home caregivers in very limited circumstances. But we’re now seeing small and promising changes. The Medicare Advantage program, for example, now allows plans to offer non-medical care services in the home as supplemental benefits. These benefits can include day care services, in-home support services including meals and support for caregivers.
We have also seen a surge of technologies to enable home-based care. From those receiving home infusion therapies, to home dialysis, to remote patient monitoring, the private sector has stepped up to meet the needs of those wanting to or needing to receive care at home.
Now is the time to expand on these promising changes with a more comprehensive approach to paying for home-based care delivery. With more thoughtful integration of caregiving services and improved care coordination across care settings, including the home, such models can drive down health care costs for patients and the system overall.
Whether caring for those impacted by our current public health crisis, or those who are medically homebound, or those who simply choose to age in place, policymakers should think beyond essential medical services and consider the non-medical drivers of health that are often as essential to good health outcomes. For example, many individuals needing to stay at home are ill-equipped to carry out their own basic needs. Daily tasks — such as getting in and out of a chair or bed, moving about the house, shopping and preparing meals, taking medications properly, bathing and dressing, and cleaning and laundry — can be a struggle for the elderly and those with serious health conditions.
Fortunately, we have millions of home health nurses and caregivers working on the front lines to care for vulnerable adults who should safely remain in their homes during this pandemic and beyond.
These workers are the foot soldiers who perform tasks such as shopping, meal preparation and assisting with mobility and personal care. Well-trained caregivers and nurses, sensitive to the time and place where patients actually live, can more readily identify and address issues that can exacerbate a person’s chronic, complex illness that may not otherwise be visible in a single visit to a traditional health care setting.
As we face record unemployment, federal, state and local policymakers should consider how best to utilize this untapped resource both now and in the future. With the appropriate testing, training, and reimbursement, individuals can have a choice in where they age and receive care.
While keeping people safe and healthy in their homes has always been appealing, now it is imperative. For our most vulnerable individuals — the elderly and those with chronic health conditions – home-based care can save their lives.
By Tom Daschle & Bill Frist | June 3, 2020
Source: MORNING CONSULT
The COVID-19 pandemic and killing of George Floyd along with other recent deaths of African American people at the hands of police have laid bare stark structural and systemic racial inequities and their impacts on the health and well-being of individuals and communities. While these events have brought health and health care disparities into sharp focus for the media and public, they are not new. These longstanding and persistent health disparities are symptoms of broader social and economic challenges that are rooted in structural and systemic barriers across sectors — including housing, education, employment, and the justice system — as well as underlying racism and discrimination. Amid this difficult time for our nation, the increased recognition and understanding of disparities could provide a catalyst for the challenging work required to address them.
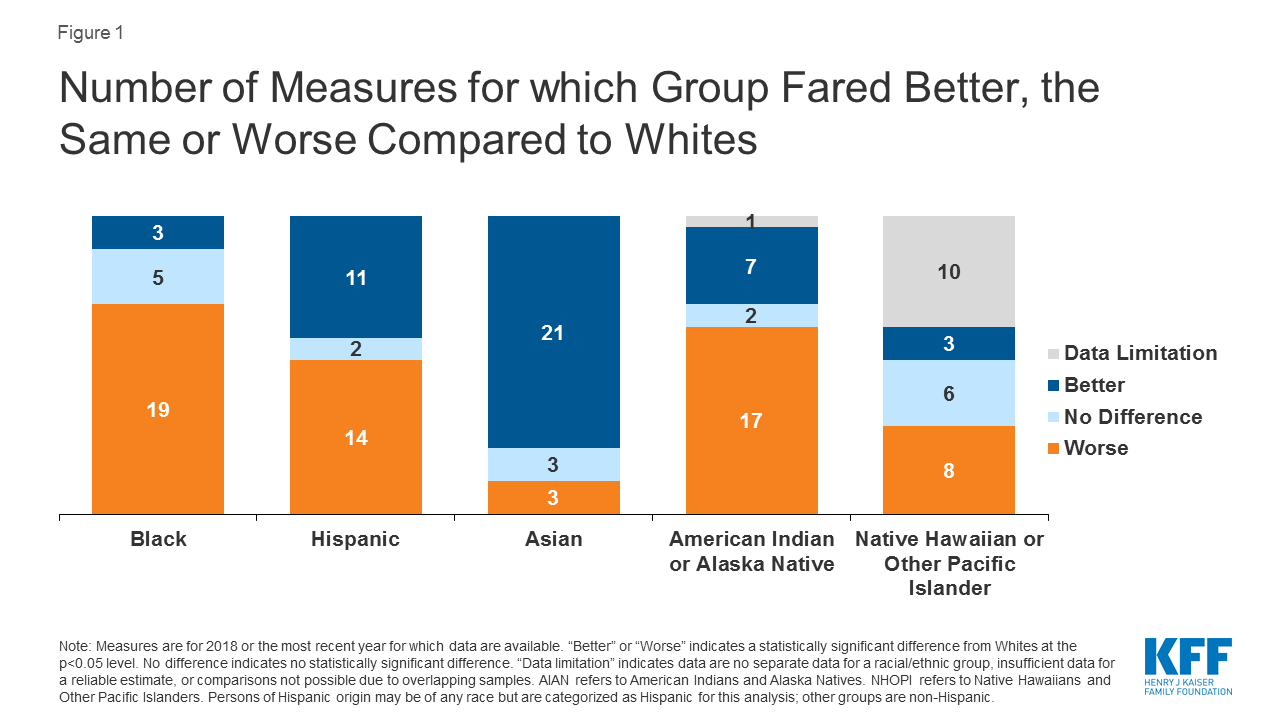
Despite being recognized and documented for many years, disparities in health and health care have persisted and in some cases widened over time. Our analysis finds that Black and American Indian or Alaska Native (AIAN) individuals continue to fare worse compared to White individuals across most examined measures of health status, including physical and mental health status; birth risks; infant mortality rates; HIV and AIDS diagnosis and death rates; and prevalence of and death rates due to certain chronic conditions (Figure 1). For example, the infant mortality rate for Black and AIAN individuals is roughly two times higher than the rate for White individuals. Black teens and adults have an over eight times higher HIV diagnosis rate and a nearly ten times higher AIDS diagnosis rate compared to their White counterparts; the HIV and AIDS diagnosis rates for Hispanic teens and adults are more than three times higher compared to the rates for those who are White.
Figure 1: Number of Measures for which Group Fared Better, the Same or Worse Compared to Whites
The disparate impacts of the COVID-19 pandemic on people of color mirror and compound these broader underlying racial/ethnic disparities in health. Data across states show that, in the majority of states reporting data, Black people account for a higher share of COVID-19-related deaths and cases compared to their share of the population. Similarly, Hispanic individuals make up a higher share of confirmed cases relative to their share of the population in most states reporting data, and there have been striking disproportionate impacts for American Indian or Alaska Native, Asian, and Native Hawaiian or Other Pacific Islander people in some states. The resulting economic crisis has also had an unequal effect on people of color.
Health disparities, including disparities related to COVID-19, are symptoms of broader underlying social and economic inequities that reflect structural and systemic barriers and biases across sectors. Though health care is essential to health, it is a relatively weak health determinant. Research shows that social determinants of health—the conditions in which people are born, grow, live, work and age—are primary drivers of health. They include factors like socioeconomic status, education, neighborhood and physical environment, employment, and social support networks, as well as access to health care (Figure 2). For example, children born to parents who have not completed high school are more likely to live in an environment that poses barriers to health such as lack of safety, exposed garbage, and substandard housing. They also are less likely to have access to sidewalks, parks or playgrounds, recreation centers, or a library. Further, evidence shows that stress negatively affects health across the lifespan and that environmental factors may have multi-generational impacts.
Figure 2: Social and Economic Factors Drive Health Outcomes
The heightened focus on and understanding of disparities can serve as a catalyst for the challenging work required to address them. Steps can be taken within the health care system that would help address health disparities. For example, actions to expand health coverage, such as adoption of the Medicaid expansion to low-income adults in the 14 states that have not yet expanded; increasing accessibility to health care providers; increasing access to linguistically and culturally appropriate care; and diversifying the health care workforce could help reduce health disparities. However, efforts to address health disparities also require cross-sector approaches beyond health care to affect the broader social and economic factors driving health. For example, actions to increase access to healthy food options and improve food security; improve affordability and quality of housing; enhance educational opportunities; improve built environments and provide more green spaces and recreational opportunities; and increase financial security and economic opportunity may all positively affect health and reduce health disparities. Beyond these factors, any effort would be woefully incomplete if it does not also recognize and address racism and discrimination and long histories of stress and trauma affecting the health of individuals and communities and how they shape our systems and policies. Such efforts are challenging and complex and require strong leadership, community engagement, resources, and cross-sector collaboration to achieve progress forward.